Antibodies derived from natural infection with COVID-19 are more abundant and more potent-at least 10 times more potent than immunity generated by vaccination alone
Originally posted on medscape.co.uk by Sheena Meredith, MB BS, MPhil, February 28, 2022
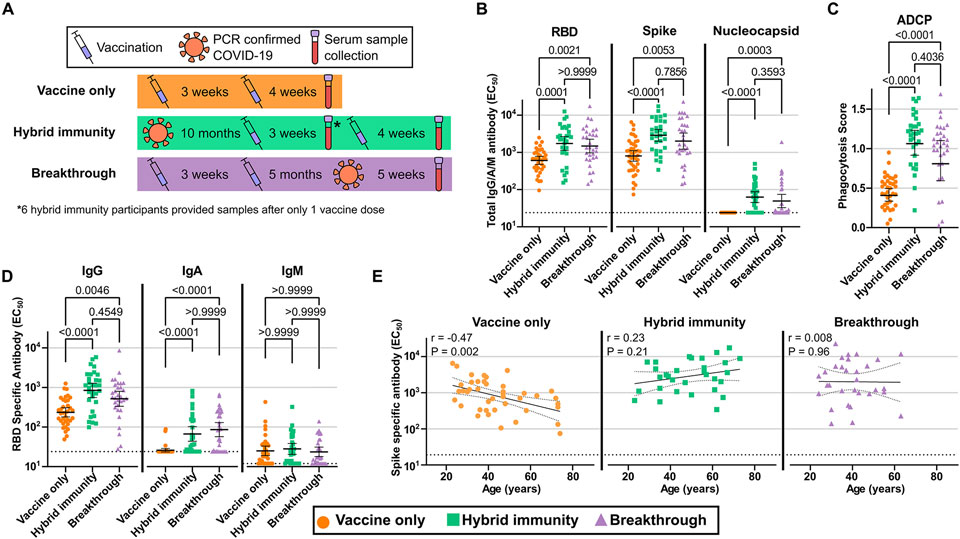
Antibodies derived from natural infection with COVID-19 are more abundant and more potent – at least 10 times more potent – than immunity generated by vaccination alone, according to a study from Oregon Health & Science University (OHSU) in Portland, US, published on January 25.
Three days later, the US Centres for Disease Control (CDC) reported in an MMWR Early Release that before Delta became the predominant variant in June 2021, case rates were higher among people who survived a previous infection than among people who were vaccinated alone. However by early October, those who had been previously infected had lower case rates than those who were vaccinated alone.
These studies focus renewed attention on the ongoing debate about the importance of infection-acquired immunity and the extent to which it should be taken into account in public health policy.
While many authorities do accept documented recovery from COVID-19 as a temporary ‘get out of jail free’ card, the allowance is generally short-lived and those who have been infected are still urged to get vaccinated.
Yet, although the OHSU study was used to conclude that the combination of vaccine with natural infection (hybrid immunity) induces a sort of ‘super-immunity’, irrespective of whether infection or vaccination comes first, there is increasing evidence that immunity derived from natural infection with COVID-19 gives powerful protection on its own. Natural immunity has been shown to be both highly protective and long lasting, and to safeguard against both re-infection and severe disease.
For example, a study in Geneva, Switzerland, of people infected in the first wave showed a 15.5% infection rate in seronegative individuals compared with just 1% in seropositives, giving overall protection attributable to infection of 94% – comparable with that in the original Pfizer vaccine trial.
Another study from India showed that seropositivity protected against both infection and severe disease, and suggested “strong plausibility that development of antibody following natural infection not only protects against re-infection by the virus to a great extent, but also safeguards against progression to severe COVID-19 disease”.
Natural infection also protects against the different variants that have arisen progressively since the start of the pandemic. A national database study including almost 22,000 people in Qatar published in the New England Journal of Medicine showed that previous infection was “robust” – approximately 90% – in preventing reinfection with the Alpha, Beta, and Delta variants of SARS-CoV-2, and approximately 60% “but still considerable” against Omicron. None of the re-infections progressed to critical or fatal outcomes and the effectiveness against severe, critical, or fatal COVID-19 was estimated to be 69.4% against Alpha, 88.0% against Beta, 100% against Delta, and 87.8% against Omicron variants.
Long-Lasting Protection
Protection from natural immunity also seems to be durable. People infected with SARS-CoV-2 in 2020 and early 2021 had around 72% to 86% protection against reinfection with the virus for at least 6 months, according to a study of US SpaceX employees partly funded by the UK National Institute for Health Research (NIHR) and published earlier this month in PLOS Biology.
A multicentre, prospective cohort of NHS workers published in the Lancet showed an 84% lower risk after natural infection lasting at least 7 months. A report from Dublin published in January this year reviewed 11 large cohort studies and found natural immunity lasted at least 10 months.
“Re-infection was an uncommon event (absolute rate 0% to 1.1%), with no study reporting an increase in the risk of re-infection over time,” the authors said.
Another study following up first wave infections in Lombardy, Italy, before the emergence of variants, also showed that re-infections were rare and protection from infection lasted at least one year. In a further Italian study of 36 patients with documented COVID-19 infection in March 2020, who were followed to Sept 2021, the 17 individuals who remained unvaccinated demonstrated persistence of IgG antibodies to at least 18 months, according to a preprint study published last month.
And most recently, a study published online in JAMA on February 3 showed antibody levels sustained up to 20 months following a positive COVID-19 test.
Broadly-speaking then, natural immunity, so far, seems generally to last for at least as long as the studies assessing it, and to offer robust protection against both re-infection and, on the rare occasions re-infection has occurred, against severe outcomes.
Comparisons With Vaccine-induced Immunity
Furthermore, a study of over 30,000 Cleveland clinic employees followed for 4 months from the start of an mRNA vaccine roll out in December 2020 found cumulative infection rates did not differ between previously infected people who were or were not subsequently vaccinated, or those uninfected who received the vaccine. Researchers concluded that those previously infected “are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before”.
This accords with the general pre-COVID view that natural infection offers superior and lasting protection from disease compared with vaccination. It is increasingly acknowledged that while COVID vaccines protect against severe disease, they do not prevent infection per se, and it is now clear that they do not stop transmission, as even the Prime Minister has acknowledged.
Moreover, vaccine-induced protection wanes quite quickly, particularly since the advent of Delta and subsequent variants. Protection from infection by 6 months was reduced to just 29% from two doses of Pfizer and 59% from two doses of Moderna, with no detectable effectiveness at all from the AstraZeneca jab from 4 months onwards, according to a large nationwide study in Sweden also published this month.
A pre-publication study from Israel to be presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases in Lisbon in April compared previously infected-unvaccinated people with double-vaccinated-never infected individuals. Results showed that, although over time the number of SARS-CoV-2 antibodies falls in both previously-infected and vaccinated patients, the performance of antibodies improves only after previous infection, and not after vaccination.
“This difference could explain why previously-infected patients appear to be better protected against a new infection than those who have only been vaccinated,” the researchers concluded.
Commenting on the study, Dr Julian Tang, a clinical virologist at the University of Leicester, said: “Generally, natural infection generates a broader and longer-lasting set of immune responses to all the viral antigens – so this is not really surprising. After all, our immune systems have evolved over several million years to deal with all types of pathogens – so I would expect natural immunity to outperform any vaccine-induced immunity over the longer term.”
Caution Over Boosters
Declining protection from what were originally billed as ‘full courses’ of vaccines, resulting in increasing so-called ‘breakthrough’ infections even in the fully-vaccinated, have led to growing recommendations for booster shots. However the latest study, published this month from the CDC, showed waning immunity against severe disease just 4 months after a third dose of an mRNA vaccine, similar to the drop in effectiveness after a second dose.
Vaccine protection waned during both Delta and Omicron waves, and has been lower overall during the Omicron period. Even vaccine manufacturers now admit the likely need for annual jabs to maintain protection. However the effectiveness of boosters has been questioned, and repeated boosters may impart unexpected dangers: last month the head of the European Medicines Agency acknowledged the potential risk of immune system overload after multiple shots.
In addition, evidence that people who have recovered from COVID-19 may experience higher rates of side effects after vaccination, possibly due to existing levels of antibodies interacting with a subsequent vaccine to create immune complex deposition, has also been largely ignored. A comparison using data from the ZOE symptom app found that both local and systemic side-effects were more common among individuals with previous SARS-CoV-2 infection than among those without known past infection (systemic side-effects 2.9 times more common after the first dose of Pfizer and 1.6 times after the first dose of the Astra vaccine).
Public Health Policy
Yet, even where authorities allow documented recovery from COVID-19 as a temporary alternative for certification purposes or for exemption from vaccine mandates, the allowance is generally limited in scope or short-lived – in Austria and in the UK to just 6 months after a positive PCR test, even though protection has been shown to last far longer. In Germany, infection is now recognised for only 3 months (down from 6 months previously), whereas in Switzerland it confers ‘honorary vaccinated’ status for a full 12 months. In Canada, recovery is not recognised at all.
Similarly in the US at national level, there is no recognition of natural immunity under CDC policy. It has been admitted that this is partly for logistic reasons – it was viewed as too complicated to test people first: “It’s a lot easier to put a shot in their arm,” according to Alfred Sommer, dean emeritus of the Johns Hopkins Bloomberg School of Public Health. It is also partly political.
The message that even if someone has had COVID-19 it’s still better to get vaccinated “is not based on data. There’s something political going on around that”, according to Monica Gandhi, an infectious disease specialist at University of California San Francisco.
Comparative studies of natural infection and vaccination are also illuminative. A study in Israel showed that protection from reinfection decreased with time since previous infection, but was still higher than that conferred by two-dose vaccination at a similar time since the last immunity-conferring event.
Another Israeli study demonstrated that natural immunity conferred longer-lasting and stronger protection against re-infection, symptomatic disease and hospitalisation caused by the Delta variant of SARS-CoV-2 compared with two-dose Pfizer/BNT vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
In the US, a pooled analysis of seven clinical studies showed “no statistical advantage to vaccination in the COVID-naive, compared with natural immunity in the COVID-recovered”. In addition: “Vaccination in the COVID-recovered may provide some incremental protective benefit, but the size of this benefit is marginal.”
The authors concluded: “COVID-recovered individuals should be considered to have at least equal protection to their vaccinated COVID-naïve counterparts… National policy should reflect the need for clinical equipoise and restraint in the decision to vaccinate these individuals by mandate.”
Back in January 2021, the CDC instructed everyone, regardless of previous infection, to get fully vaccinated as soon as they were eligible, stating on its website that natural immunity “varies from person to person” and “experts do not yet know how long someone is protected”.
Despite acknowledging some of these studies, the advice has not materially changed and still states that COVID-19 vaccination is recommended for all eligible persons, including those who have been previously infected with SARS-CoV-2.
Yet length of protection after natural infection has now proven highly durable, and more so than that of vaccines absent multiple boosters. There is an increasingly strong argument that at the very least the protection afforded by natural infection might be acknowledged by allowing just one vaccine dose in the previously-infected. “This would also spare individuals from unnecessary pain when getting the second dose and it would free up additional vaccine doses,” according to virologist Florian Krammer of the Icahn School of Medicine at Mount Sinai, New York.
Such a policy is supported by a study part-funded by the US National Institutes of Health showing that whereas previously uninfected people reach peak immunity after a second vaccine dose, those who have recovered from previous infection reach peak immunity after the first dose. “A second dose… may be not necessary in individuals previously infected with SARS-CoV-2,” the authors concluded.
This is the approach taken in the EU, where the digital COVID certificate can be issued after a single dose of an mRNA vaccine to people who have had a positive test result within the previous 6 months, although again the concession is time-limited.
NHS Staff Opposed to Mandates
However, such dispensations may not sway those healthcare workers prepared to lose their jobs rather than be vaccinated at all – one example of the unintended consequences of vaccine mandates. After 40,000 care workers were fired in November for refusing the jab, the potential loss of more crucial personnel at a time when there are already staff shortages provoked considerable concern and outright opposition from many national bodies, before Health Secretary Sajid Javid’s 11th hour row back on the NHS vax mandate.
Despite current attempts to woo back staff who resigned over the mandate, there are continuing pressures. Mr Javid – who had already asked professional regulators to conduct “urgent” reviews of their guidance on vaccination against occupational diseases, including COVID – immediately switched to urging the GMC to remind doctors of their duty to be vaccinated. A joint statement in response from the GMC and the Academy of the Medical Royal Colleges continued to urge doctors to get vaccinated, but stopped short of threatening disciplinary procedures. However senior NHS managers have been writing to staff telling them it is their “professional responsibility” to be vaccinated, and the NHS England medical director has warned that staff who remain unvaccinated against coronavirus could have this used against them in fitness-to-practise cases.
Many NHS staff worked with COVID patients all the way through the first wave – at personal risk and often with inadequate PPE – and thereby contracted infection in significant numbers. This underpinned at least some of the resistance to the mandate. Steve James, the ICU consultant whose on-camera encounter with Savid Javid attracted widespread media attention, told Mr Javid: “I’ve got antibodies, and I’ve been working on COVID ICU since the beginning… The protection I’ve got from transmission is probably equivalent to someone who’s vaccinated.”
Similarly, Dr Simon Fox, an NHS consultant in infectious diseases, has also spoken publicly about his unwillingness to be vaccinated. “Given I’ve had the infection and worked with patients with COVID for two years, I can hand-on-heart say I’m as immune as anyone else can claim to be,” Dr Fox told TalkRADIO at the end of January.
Both doctors, and others like them who feel the same way, have had extensive experience of treating the most serious COVID cases. They might reasonably expect that their professional assessment at least merits consideration. Moreover, like almost all those working in the health service, they will likely have been vaccinated against hepatitis B (although notably this is not a legal ruling), and have had, and advocated, most other vaccines. They are not ‘anti-vaxxers‘.
Ethics and Science
Yet, the protection afforded by natural immunity is still not acknowledged in policy responses, and NHS staff opposing the mandate have described its dismissal as “irrational”.
It also raises ethical questions over and above those of mandates and certifications generally. Is it justified to pressure people with pre-existing infection-acquired immunity to take a vaccine they neither want nor need? How can such individuals give proper informed consent, especially when they may be also at a higher than average risk of side-effects? Is it equitable to give unnecessary doses when vaccines have yet to be equally shared on a global level?
Moreover, the Government has repeatedly invoked ‘the science’ to reinforce coronavirus measures. Is inconvenient scientific evidence now being side-lined? Marty Makary, professor of health policy and management at Johns Hopkins University told the BMJ in an interview last September: “Public health officials… talk about the vaccinated and the unvaccinated. If we want to be scientific, we should talk about the immune and the non-immune.”
So, should we at least give recognition to the equivalent and possibly superior status of natural immunity by giving those who have been infected an exemption from vaccine requirements? And if not, why not?